
The COVID-19 pandemic has forced us to remain physically distant from each other but has also created new opportunities for us to remain socially connected. Since UNC-Chapel Hill (UNC) closed its campus in mid-March, I (Alexis) have virtually collaborated with my colleagues in the Sociology Department and at the Carolina Population Center, participated in global dance parties on Instagram, laughed with friends on Google Hangout, and played pub-style trivia over Zoom. Each week, I look forward to virtual Sunday dinner with my family in Atlanta. My parents, sister, and I coordinate the time we will finish cooking, sit at our respective tables, and share the week’s joys, fears, and struggles. Through these conversations, I noticed differences in the policy responses to the coronavirus pandemic unfolding in NC and GA, and I worried these policy differences would have dire health consequences for the populations of these states.
Watching this pandemic unfold has both professional and personal implications for me: I am an advanced doctoral student in the Sociology Department who studies racial, socioeconomic, and gender disparities in health across the early life course. At UNC I am lucky to train under a renowned mortality demographer, Dr. Robert Hummer, and an esteemed social epidemiologist with expertise in global pandemics, Dr. Allison Aiello. Prior to returning for doctoral training, I worked in HIV and mental health research at UNC, FHI-360, and the Duke Global Health Institute.
I am also an African American woman who was raised by two hardworking parents who are on the cusp of retirement and in the high-risk category for COVID-19. In my research, I examine how the social structure of societies facilitates the emergence of health disparities along lines of race and socioeconomic status. As such, I expected for disparities to emerge in coronavirus infections and mortality as the pandemic unfolds in the US. Despite my knowledge of population health, I was somewhat unprepared for the emotional impacts of seeing my expectations confirmed. The first reports of high COVID-19 mortality among African Americans in New York, Milwaukee, and Chicago made me very concerned about my own family’s health, safety, and wellbeing.
Despite this concern, I was also curious: would the differences in NC and GA policies show up in the data? This was apparent to me anecdotally in the way the two states differed in their approach to shutting down and reopening. For example, on March 11th when UNC announced the transition to remote learning, my mom and sister were still going into the office each day. Towards the end of March when Gov. Roy Cooper issued a stay-at-home order for NC residents, my parents, home in Georgia, shared that our longtime friends from church both had COVID-19 and were recovering at home after a brief hospitalization. During Sunday dinner on April 19th – the day before Georgia’s Gov. Brian Kemp announced plans to re-open GA – my parents described the graveside virtual funeral they attended that weekend. Our family friend passed from complications due to COVID-19.
NC and GA both reported their first coronavirus cases in early March. At that time, state officials may have interpreted the few cases as not warranting aggressive action. On the other hand, community transmission of coronavirus was likely occurring before the CDC expanded testing eligibility and before states could access large quantities of [working] diagnostic tests. Understanding that the coronavirus was likely spreading faster than the “data” would warrant early, aggressive, containment action, which would in turn, reduce infections and mortality. As a bystander, North Carolina’s response to the coronavirus pandemic seemed more aggressive and data-driven than Georgia’s.
I shared my family’s experiences in GA with my friend from graduate school, Nathan. Nathan is a doctoral candidate in the Sociology Department who studies mortality and immigration. We reviewed the timing of mitigation measures, such as school closures and stay-at-home orders enacted by North Carolina and Georgia and report our findings in Table 1, below. We also decided to dig into some data and examine whether my instincts about geographic differences in coronavirus mortality were correct.
Table 1 suggests North Carolina consistently acted earlier than Georgia to prepare for and mitigate the spread of coronavirus. For example:

download PDF with media links: Here
Given Georgia and North Carolina’s different policy responses to coronavirus, we were interested in answering two research questions:
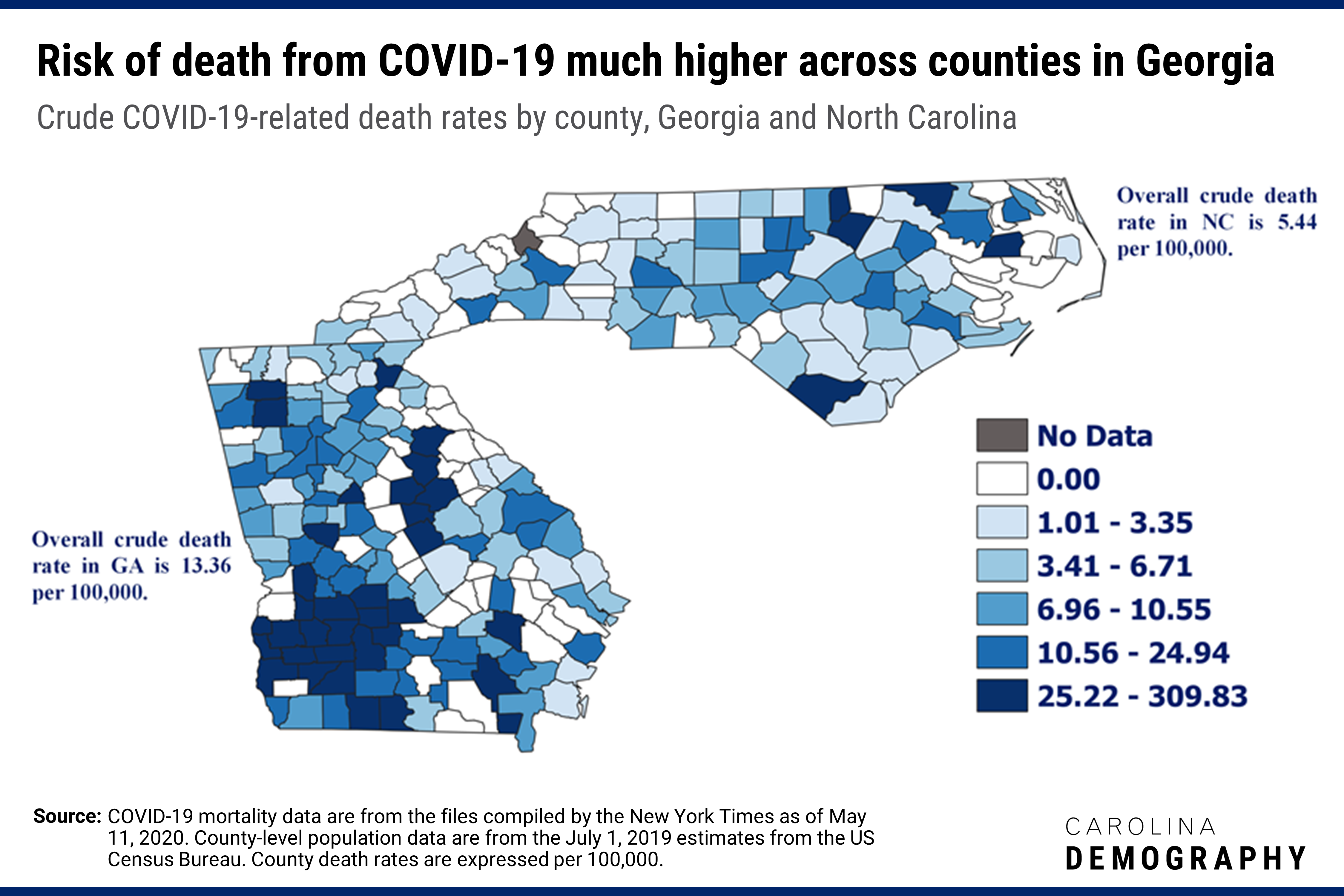
To answer these questions, we merged county-level COVID-19 mortality data compiled by The New York Times as of May 11, 2020 with July 1, 2019 county population estimates from the US Census Bureau found here. Using the total number of COVID-19-related deaths in each county as our numerator, and county population estimates as our denominator, we calculated the crude mortality rates from COVID-19 for each of the 259 counties in NC (100 counties) and GA (159 counties). We were interested in whether GA counties have experienced higher crude mortality due to COVID-19 than counties in NC, which we might expect given the contrast in policy responses to the pandemic between NC and GA. In the figure below, we map the crude COVID-19-related mortality rate for each county. The 65 counties reporting zero deaths appear in white and the one county (Avery County, NC) with no data appears in gray. The remaining counties are broken down into quintiles (5 equal groups). The crude rates for the 259 counties are broken into quintiles with darker shades representing higher mortality rates.
It is clear from the map that the risk of death from COVID-19 is considerably higher in GA compared to NC. Overall, the crude mortality rate in GA is 13.36 per 100,000, 2.5 times higher than the overall crude mortality rate in NC (5.44 per 100,000). Among the 38 counties in the fifth and highest quintile, with a crude mortality rate ranging from 25.22-309.83 per 100,000, 33 counties or 87%, are in GA. To put these numbers in context, the overall US crude mortality rate due to influenza and pneumonia in 2017 was 17.1 per 100,000. Even more striking, 9 counties in GA (Clay, Dougherty, Early, Mitchell, Randolph, Sumter, Terrell, Turner, and Wilcox) currently have crude mortality rates from COVID-19 above 100 per 100,000, and three of those counties (Early, Randolph, and Terrell) have rates above 200 per 100,000.
The majority of the counties in GA with the highest risk of death from COVID-19 are in the southwestern part of the state – rural counties that tend to be the poorest and have the highest concentrations of African Americans in the state. For example, the highest rate of death of any county in GA and NC is found in Randolph County, GA (309.83 per 100,000) where, according to 2018 American Community Survey data, 62% of the population is African American and 29% of families live below the poverty line. In NC, we see a similar clustering of counties with the highest risk of death from COVID-19. With a few exceptions in the western part of NC (Burke and Henderson Counties), the highest risk of death from COVID-19 is found in counties in the eastern part of the state, primarily along the I-95 corridor—counties, which also tend to be the poorest and have the highest concentrations of African Americans in the state.
The disparate COVID-19 mortality observed in the GA and NC counties that are poorest and have the highest concentrations of African Americans track with media reports that African Americans are disproportionately dying from COVID-19 across the U.S. Population and public health research suggests that African Americans experience chronic low-grade stress and accelerated biological aging in response to exposure to structural/institutional and interpersonal racism. Accelerated biological aging is associated with the early onset of chronic diseases, including diabetes and cardiovascular disease, as well as more severe illnesses, and premature mortality. Historic discrimination in health care, education, housing, and employment also make African Americans more likely than Whites to be uninsured, to have poor access to quality health care, to live in racially and socioeconomically segregated neighborhoods, to be exposed to environmental toxins, and to work in occupations that have been deemed “essential” during the coronavirus pandemic today.
It is important to interpret the data and analyses presented here with caution. For example, crude mortality rates do not account for age differences that drive mortality. Moreover, additional research is necessary to better understand how COVID-19 is disparately impacting individuals, families, and communities along lines of race and socioeconomic status in Georgia and North Carolina. Despite these limitations, we provide preliminary evidence that state differences in policy response contributed to lower COVID-19 mortality rates observed across counties in North Carolina.
While national and local media have been very attentive to COVID-19 disparities in urban areas, our analysis highlights the need to be attentive to COVID-19 mortality disparities emerging in rural communities, low resourced communities, and communities of color.
In addition, our findings underscore the importance for NC leaders to not only consider trends in COVID-19 incidence, prevalence, and mortality rates in North Carolina, but to also examine trends in neighboring states as we consider the potential impact of moving into Phase II of reopening by the end of this week.
Alexis C. Dennis, MA, MPH is a doctoral candidate in the Department of Sociology and a Pre-doctoral Trainee at the Carolina Population Center.
Nathan T. Dollar, MA, MA is a doctoral candidate in the Department of Sociology and a Pre-doctoral Trainee at the Carolina Population Center.
Need help understanding population change and its impacts on your community or business? Carolina Demography offers demographic research tailored to your needs.
Contact us today for a free initial consultation.
Contact UsCategories: Health & Environment, NC in Focus
Tags: COVID-19

The Center for Women’s Health Research (CWHR) at the University of North Carolina School of Medicine released the 12th edition of our North Carolina Women’s Health Report Card on May 9, 2022. This document is a progress report on the…
Dr. Krista Perreira is a health economist who studies disparities in health, education, and economic well-being. In collaboration with the Urban Institute, she recently co-led a study funded by the Kate B. Reynolds Foundation to study barriers to access to…

Our material helped the NC Local News Lab Fund better understand and then prioritize their funding to better serve existing and future grant recipients in North Carolina. The North Carolina Local News Lab Fund was established in 2017 to strengthen…
Your support is critical to our mission of measuring, understanding, and predicting population change and its impact. Donate to Carolina Demography today.